Table of Contents
Introduction
West Nile fever isn’t something most people think about until they’re swatting mosquitoes at a backyard barbecue. Then one day, a headline pops up. Someone in your county tested positive. Suddenly it feels a lot more real.
This article covers everything — from what West Nile fever actually is, how the virus spreads, what symptoms look like, how it’s treated, and how you can protect yourself and your family. Whether you’re looking for fast answers or a deep dive, you’re in the right place.
What Is West Nile Fever?
West Nile fever is an infection caused by the West Nile virus, a single-stranded RNA virus from the Flaviviridae family — same family as dengue and Zika, if you want some context. It was first identified in Uganda back in 1937, in the West Nile district (hence the name). For decades, it stayed mostly in Africa, the Middle East, and parts of Europe.
Then 1999 happened. The virus showed up in New York City and within a few years had spread across the entire continental United States. That’s not an exaggeration — it’s now the most common mosquito-borne illness in the US.
Most people who get infected — roughly 80% — never develop symptoms at all. About 1 in 5 develop West Nile fever. A smaller group, less than 1%, develops severe neurological disease. That smaller group is the one that scares doctors.
West Nile Fever vs West Nile Virus: Is There a Difference?
People use these terms almost interchangeably, and honestly, the confusion is understandable. Here’s the technical breakdown:
| Term | What It Means |
|---|---|
| West Nile Virus (WNV) | The actual pathogen — the virus itself |
| West Nile Fever | A clinical syndrome caused by WNV — fever, aches, rash |
| West Nile Neuroinvasive Disease | Severe form — meningitis, encephalitis, flaccid paralysis |
| Asymptomatic WNV Infection | Infected but no symptoms — ~80% of cases |
So, West Nile fever is what you get when the virus causes noticeable illness but doesn’t invade the brain or spinal cord. West Nile virus is the broader term. Most people searching ‘West Nile fever’ are asking about the milder, more common form — that’s what we’ll focus on, while covering the serious stuff too.
A Brief History of West Nile Fever
The virus was first isolated from a woman in the West Nile district of Uganda in 1937. It circulated quietly in Africa and Asia for decades. Occasional outbreaks occurred in Israel and parts of Europe in the 1950s and 60s.
The big turning point — at least for Americans — was the 1999 New York outbreak. Birds started dying mysteriously in the Bronx Zoo. People in Queens got sick with encephalitis. The CDC and New York City health officials eventually connected the dots. West Nile virus had jumped continents.
Nobody’s entirely sure how it got here. The leading theory involves an infected bird or mosquito arriving via international travel or cargo. Whatever the route, once it arrived, it spread fast. By 2003, it had reached the Pacific Coast. By 2012, the US experienced one of its worst outbreaks ever — over 5,000 cases reported, and the real number was likely far higher.
Understanding this history matters because it shows how quickly a mosquito-borne virus can establish itself. And it should make us take prevention seriously.
Which Mosquito Causes West Nile Fever?
The Primary Culprit: Culex Mosquitoes
West Nile fever is caused by which mosquito? The answer is mainly Culex species — specifically Culex pipiens in the northern US and Culex quinquefasciatus in the South. These are different from the Aedes mosquitoes that spread Zika or dengue.

Culex mosquitoes have some habits that make them particularly effective at spreading the virus:
- They bite mostly at dusk and dawn (though some bite at night)
- They breed in stagnant water — gutters, birdbaths, old tires, neglected flower pots
- They feed on both birds and humans, making them ideal virus bridges
- They don’t need much water — even a bottle cap of standing water can host larvae
Birds are the primary reservoir hosts. Mosquitoes pick up the virus by feeding on infected birds, then transmit it to humans. Humans are what epidemiologists call ‘dead-end hosts’ — we don’t have high enough viral loads to infect the next mosquito that bites us. The chain stops with us.
West Nile Fever Transmission: How Does It Spread?
How Is West Nile Fever Transmitted?
The vast majority of human infections — over 99% — come from the bite of an infected Culex mosquito. That’s the primary transmission route, full stop. But there are a few other documented (though rare) ways West Nile fever is transmitted:
- Mosquito bites — by far the most common route
- Blood transfusions — rare, screening now in place in the US
- Organ transplants — documented cases, recipients can be infected by donor organs
- Mother to child — possible during pregnancy, delivery, or breastfeeding
- Laboratory exposure — extremely rare, occupational hazard for researchers
You cannot get West Nile fever from touching an infected person, from a cough, or from casual contact. It’s not contagious person-to-person. That’s an important point — and one that gets misunderstood.
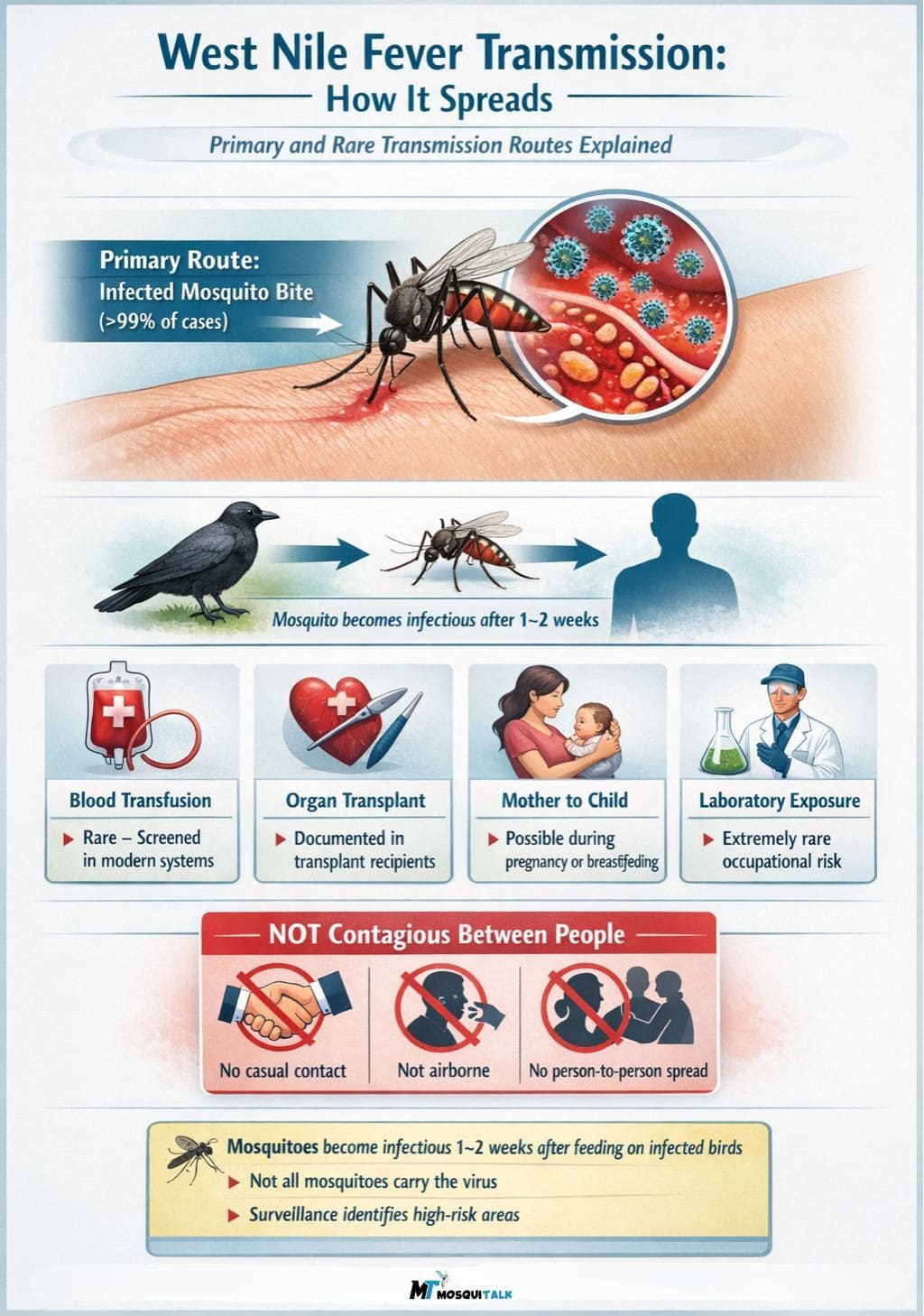
Image Credit: Illustration by Author
West Nile Fever Incubation Period
After an infected mosquito bites you, how long before you feel sick? The West Nile fever incubation period is typically 2 to 14 days. Most people who develop symptoms start feeling them within 3 to 7 days.
This window matters for a few reasons. If you’ve been in a high-risk area and start feeling flu-like symptoms within two weeks, that’s your cue to contact a healthcare provider and mention the possible exposure. Don’t assume it’s just a regular cold.
West Nile Fever Symptoms: What to Watch For
1. What Are the Symptoms of West Nile Fever?
About 20% of people infected with the virus develop West Nile fever. Symptoms can range from mild to quite miserable. Here’s what typically shows up:
| Symptom | Details |
|---|---|
| Fever | Usually 100-103°F; can be higher |
| Headache | Often described as severe, front of head |
| Body aches | Muscle pain, joint stiffness, fatigue |
| Nausea / vomiting | Especially in first few days |
| Rash | Skin rash on trunk and limbs — see below |
| Swollen lymph nodes | Particularly in neck, armpits |
| Eye pain | Sensitivity to light, eye soreness |
2. West Nile Fever Rash: What Does It Look Like?
The West Nile fever rash is one of the more distinctive features. It typically appears as a maculopapular rash — small, flat or raised red spots that can merge into larger patches. It usually shows up on the trunk (chest, back, abdomen) and can extend to the arms and legs. The face is generally spared.
West Nile fever rash pictures in medical literature show a pattern that can look similar to rashes from other viral illnesses — which is part of why diagnosis can be tricky without lab confirmation. The rash tends to appear a few days into the illness and may last several days.
Not everyone gets the rash. Studies suggest it appears in about 20–50% of people with West Nile fever. If you see an unexplained rash alongside fever and body aches during summer months, get it checked.
3. How Long Does West Nile Fever Last?
Most people recover from West Nile fever within a few days to a couple of weeks. The fever itself usually breaks within 3–5 days, but fatigue can drag on for weeks — sometimes months. That post-illness fatigue is real, and it’s frustrating for patients who expect to bounce back quickly.
How long does West Nile fever last overall? Mild cases: 3 to 7 days. Some people experience lingering symptoms — weakness, memory problems, difficulty concentrating — for months after recovery. This is more common in older adults.
West Nile Fever Complications: When It Gets Serious
Here’s where things get more sobering. For most healthy adults under 50, west nile fever is miserable but not life-threatening. But for older adults, people with weakened immune systems, and those with certain underlying conditions, the virus can invade the central nervous system. This is called West Nile neuroinvasive disease.
The three main forms of West Nile neuroinvasive disease are:
- West Nile meningitis — inflammation of the membranes surrounding the brain and spinal cord
- West Nile encephalitis — inflammation of the brain itself; can cause confusion, seizures, coma
- West Nile acute flaccid paralysis — sudden muscle weakness resembling polio; can affect breathing
Approximately 1 in 10 people who develop neuroinvasive disease will die. Many survivors have long-term neurological effects. Age is the biggest risk factor — the older you are, the higher the risk.
How Is West Nile Fever Diagnosed?
It’s not as simple as a rapid test. Diagnosis involves a combination of clinical assessment and lab work:
- Clinical history — recent mosquito exposure, geographic area, timing of illness
- Blood tests — serology to detect IgM antibodies against WNV (ELISA test)
- Cerebrospinal fluid (CSF) analysis — if neurological symptoms are present, a lumbar puncture may be done
- PCR testing — can detect viral RNA in blood or CSF, but window is short
- MRI or CT scans — used to evaluate brain involvement in severe cases
The IgM antibody test is the workhorse of WNV diagnosis. Antibodies typically become detectable within 3–8 days of symptom onset and can persist for months. One complication: cross-reactivity with other flaviviruses (like dengue or Zika) can create false positives, so clinical context matters.
Many mild cases are never formally diagnosed — people recover thinking they had a bad flu. This is why official case counts dramatically underrepresent actual infections.
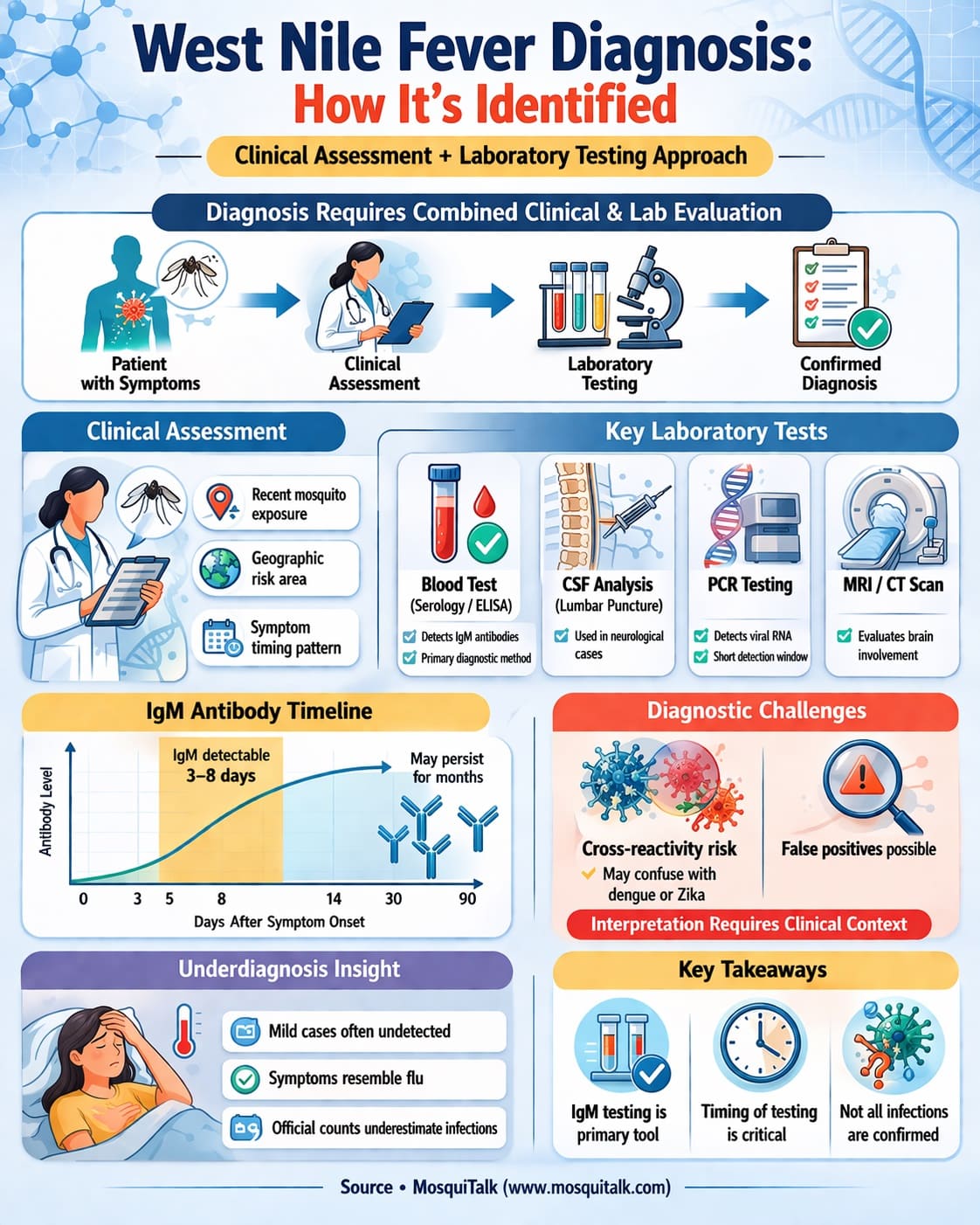
Image Credit: Illustration by Author
West Nile Fever Treatment: What Actually Helps?
Here’s the hard truth: There is no specific antiviral drug approved for West Nile fever. No pill you can take that kills the virus. Treatment is what doctors call ‘supportive care’ — managing symptoms while your immune system does the heavy lifting.
1. For Mild West Nile Fever
- Rest — your body needs it, seriously
- Fluids — stay well hydrated, especially with fever
- Acetaminophen or ibuprofen — for fever and pain management
- Cool compresses — can help with discomfort from fever
2. For Severe / Neuroinvasive Disease
- Hospitalization — often required for IV fluids and close monitoring
- Respiratory support — may be needed if breathing is affected
- Seizure management — anticonvulsants if needed
- Physical rehabilitation — often necessary after acute phase
Researchers have investigated several antivirals and immunoglobulins. Ribavirin, interferon, and IVIG have all been studied — results have been mixed and none are currently standard of care. Clinical trials are ongoing.
West Nile Fever Vaccine: Where Are We in 2025?
There is currently no approved West Nile fever vaccine for humans. That’s the straightforward answer.
There is an approved vaccine for horses — WNV is a major cause of encephalitis in equines, and equine vaccines have been available since 2003. But humans are still waiting.
Several vaccine candidates have gone through clinical trials over the years. DNA vaccines, chimeric live-attenuated vaccines, and subunit vaccines have all been explored. Progress has been slower than many hoped, partly because WNV follows seasonal and geographic patterns that make large-scale efficacy trials challenging.
As of 2025, no human WNV vaccine has completed Phase 3 trials with regulatory approval. Research is ongoing, and the success of COVID-19 mRNA vaccine platforms has renewed interest in applying similar technology to WNV.
West Nile Fever Prevention: What Actually Works
1. Personal Protection Strategies
Until there’s a vaccine, prevention means mosquito avoidance. It sounds basic, but the evidence clearly supports these interventions:
- Use EPA-registered insect repellents — DEET (20–30%), picaridin, IR3535, or oil of lemon eucalyptus are all effective
- Wear long sleeves and pants during peak mosquito hours (dusk to dawn)
- Install or repair window and door screens
- Eliminate standing water around your home — gutters, birdbaths, plant trays, tarps, buckets
- Change water in birdbaths weekly — Culex larvae need about 7–10 days to mature
- Use larvicides (like Bti — Bacillus thuringiensis israelensis) in standing water that can’t be drained
- Stay aware of local WNV activity — your local health department or CDC ArboNET posts surveillance data
2. Community-Level Prevention
- Municipal mosquito control programs — adulticiding and larviciding
- Dead bird surveillance — sick or dead crows and other corvids are early warning signals
- Blood supply screening — FDA-mandated since 2003
- Public education campaigns — peak season reminders (July–September)
Who Is Most at Risk for Severe West Nile Fever?
Risk factors for developing severe disease include:
- Age over 65 — the single biggest risk factor
- Organ transplant recipients — immunosuppressed by necessity
- Cancer patients on chemotherapy
- HIV/AIDS patients
- Diabetes — may increase severity
- Hypertension — associated with worse neurological outcomes in studies
Geography matters too. States with high WNV activity historically include California, Texas, Colorado, Louisiana, and Mississippi. But cases have been documented in every contiguous state — no region is completely safe during mosquito season.
The Takeaway: Don’t Wait for Symptoms to Act
West Nile fever is preventable. Not with a vaccine — not yet — but with smart, consistent habits. The mosquito that bites you at dusk on a Tuesday in August doesn’t care that you feel fine right now.
The research is clear: repellents work. Eliminating standing water works. Being aware of your local WNV activity helps you make better decisions during peak season.
If you’ve personally dealt with West Nile fever — or know someone who has — we’d genuinely like to hear about it. Drop your experience in the comments below. Was the diagnosis delayed? What helped you recover? Your story might help someone else recognize what they’re dealing with faster than you did.
And if this article helped you understand something you didn’t before — share it. Awareness is its own form of prevention.
Frequently Asked Questions (FAQs)
Q. Can you get West Nile fever more than once?
Yes, technically — but it’s uncommon. Infection typically generates lasting immunity against the specific strain. Some evidence suggests prior infection may provide cross-protection against related strains.
Q. Is West Nile fever contagious between people?
No. You cannot catch it from an infected person through casual contact. It requires a mosquito vector. Blood transfusion and organ transplant are the only documented human-to-human routes.
Q. Can pets get West Nile fever?
Dogs and cats rarely become ill from WNV, but horses are highly susceptible. If you have horses, vaccination is strongly recommended.
Q. Should I see a doctor if I think I have West Nile fever?
If you have mild symptoms and are under 50 with no underlying conditions, rest and self-care may be appropriate — but call your provider to discuss. If you’re older, immunocompromised, or have neurological symptoms, seek medical attention promptly.
References & Sources
- Centers for Disease Control and Prevention (CDC). West Nile Virus. cdc.gov/west-nile-virus/
- World Health Organization (WHO). West Nile Virus Fact Sheet.
- Nash D, et al. The outbreak of West Nile virus infection in the New York City area in 1999. NEJM. 2001.
- Petersen LR, et al. West Nile Virus: Review of the Literature. JAMA. 2013.
- Hayes EB, et al. Epidemiology and transmission dynamics of West Nile virus disease. Emerg Infect Dis. 2005.
- CDC ArboNET — CDC’s national arboviral surveillance system (updated annually)
- FDA guidance on blood supply screening for WNV (2003 onward)