Table of Contents
Introduction to West Nile Virus
I remember the summer it hit our neighborhood. A neighbor two houses down — healthy, mid-50s, a guy who jogged every morning — ended up in the hospital for nearly two weeks. West Nile virus. None of us had thought much about it before then. We swatted mosquitoes, complained about the heat, and went on with our lives. After that summer, I started paying very close attention.
West Nile virus is the most widespread mosquito-borne disease in the United States, and yet it remains deeply misunderstood by most people. Some think it’s rare. Others assume it only affects people in tropical climates. Neither is true. Every year, across the US, thousands of people are infected — and the majority of them don’t even know it. That’s part of what makes this virus so unsettling.
This guide covers everything you need to know: what the virus actually does inside your body, the full range of west nile virus symptoms, who faces the greatest danger, and — most importantly — the practical, science-backed strategies that actually work to protect yourself and your family.
What Is West Nile Virus and How Does It Spread?
West Nile virus (WNV) is a flavivirus — same family as Zika, dengue, and yellow fever. It was first identified in Uganda in 1937. For decades it stayed largely in Africa, parts of Europe, and the Middle East. Then in 1999, it arrived in New York City. By 2003 it had spread across the continental United States. That’s an extraordinary geographic expansion in a very short time.
West Nile Virus Transmission Cycle: Birds, Mosquitoes, and Humans
The virus circulates primarily between birds and mosquitoes. Birds are the reservoir hosts — they carry high viral loads in their blood without necessarily showing symptoms (though it kills some species, particularly corvids like crows and jays). Mosquitoes, especially Culex species, pick up the virus when they feed on infected birds.
Humans and horses are what epidemiologists call dead-end hosts. When an infected mosquito bites us, the virus enters our bloodstream — but our viral loads are generally too low to infect another mosquito that bites us afterward. We don’t continue the transmission cycle. Small comfort, maybe, but worth understanding.
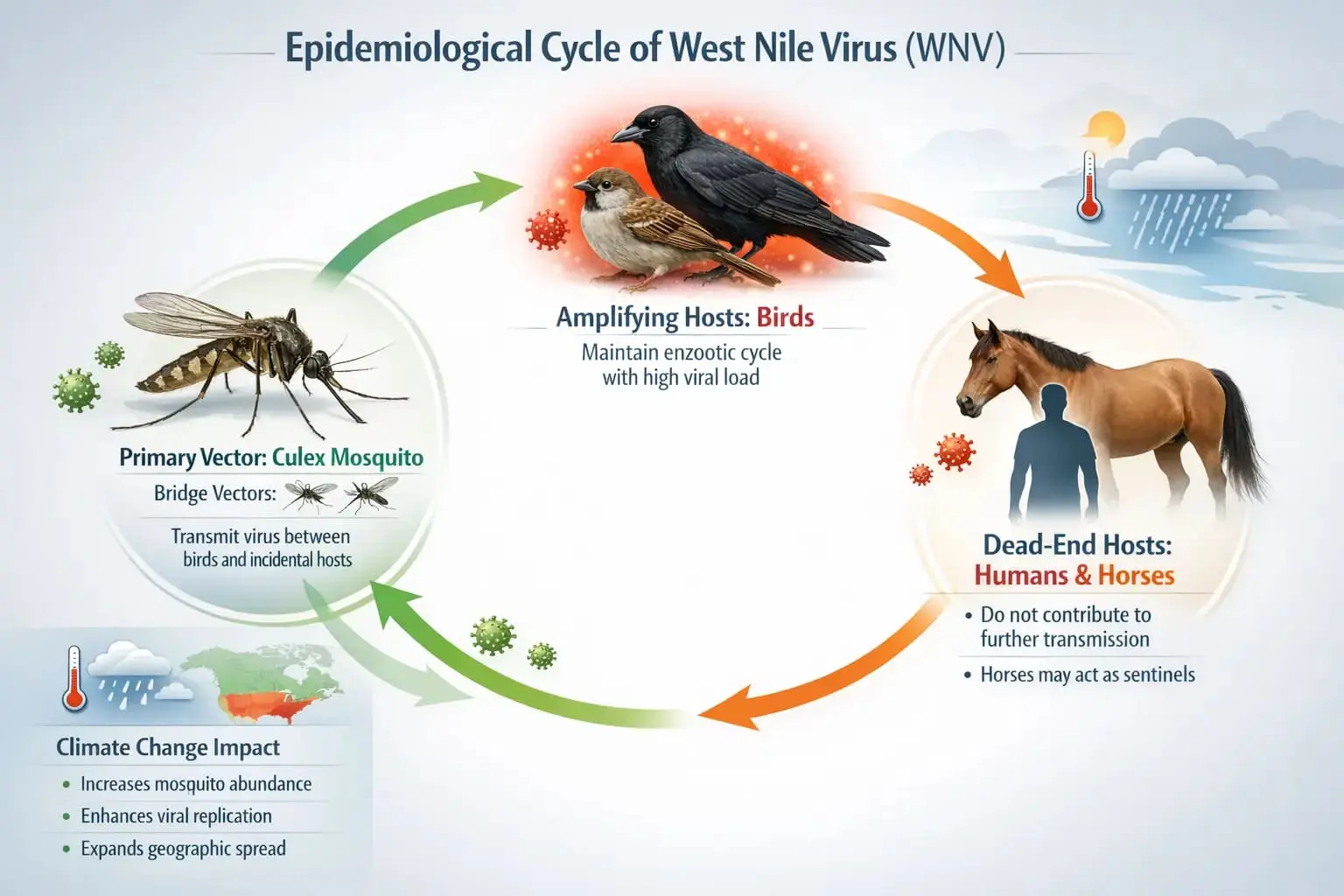
How West Nile Virus Spreads:
The Transmission Cycle
WNV circulates between birds (reservoir hosts) and Culex mosquitoes. Humans and horses are incidental dead-end hosts — the cycle cannot continue through us.
infected bird → acquires virus
bird → transmits virus
(dead-end hosts)
Source: CDC; Komar et al. (2003) Emerging Infectious Diseases; Petersen & Roehrig (2001) Annals of NY Academy of Sciences
Can You Get West Nile Virus Without a Mosquito Bite?
In rare cases, yes. The CDC has documented transmission through blood transfusions, organ transplantation, and — though very rarely — from mother to child during pregnancy or breastfeeding. There was a period before 2003 when blood screening wasn’t yet in place; since then, blood banks in the US routinely test donations. Person-to-person transmission through casual contact simply does not happen.
West Nile Virus Symptoms: What Does West Nile Virus Do to the Body?
Here’s the statistic that surprises most people: roughly 80% of people infected with West Nile virus experience no symptoms at all. Their immune systems fight off the virus without any obvious illness. But that doesn’t mean the infection is harmless across the board — not even close.
The Three Clinical Presentations of West Nile Virus (WNV)
| Category | % of Infections | Symptoms | Duration |
|---|---|---|---|
| Asymptomatic | ~80% | None — no noticeable illness | N/A |
| West Nile Fever | ~20% | Fever, headache, body aches, fatigue, rash, swollen lymph nodes | 3–6 days |
| Neuroinvasive Disease | <1% | Encephalitis, meningitis, acute flaccid paralysis | Weeks to months; may be permanent |
West Nile Virus — What Happens After Infection?
Breakdown of the three clinical presentations across all reported WNV infections
While neuroinvasive disease affects fewer than 1% of infections, adults over 70 are 43× more likely to develop it compared to those under 50.
Source: CDC West Nile Virus Surveillance Data; Hayes et al., Emerging Infectious Diseases (2005)
1. Symptoms of West Nile Fever
West Nile fever is what most symptomatic patients experience. It comes on fairly suddenly — usually 2 to 14 days after the mosquito bite. The incubation period matters because people often can’t connect their illness back to a specific bite. The symptoms of West Nile virus at this stage include:
- High fever — often 101°F to 104°F
- Severe headache, particularly behind the eyes
- Body aches and joint pain
- Profound fatigue — the kind that keeps you flat in bed
- Nausea and occasional vomiting
- Skin rash on the trunk (in about half of patients)
- Swollen lymph nodes
Most people recover fully within a week. But a subset — especially older individuals — continue experiencing fatigue and weakness for weeks or even months afterward. Post-infectious fatigue is more common with West Nile than many physicians initially acknowledged.
2. Symptoms of West Nile Virus Neuroinvasive Disease: The Serious Face of WNV
This is the version that hospitalizes people. Less than 1% of infections progress to neuroinvasive disease, but when they do, the consequences can be severe and lasting. What does West Nile virus do at this level? It crosses the blood-brain barrier and causes inflammation in the central nervous system. Three distinct syndromes emerge:
- West Nile Encephalitis — inflammation of the brain tissue itself. Confusion, disorientation, tremors, seizures. This is the most dangerous form.
- West Nile Meningitis — inflammation of the membranes surrounding the brain. Stiff neck, severe headache, sensitivity to light, fever.
- Acute Flaccid Paralysis (AFP) — a polio-like syndrome where the virus attacks motor neurons. Limb weakness or paralysis can be sudden and, in some patients, permanent.
How to Know If You Have West Nile Virus: Diagnosis and Testing
This is genuinely tricky. The symptoms of West Nile virus — fever, headache, fatigue — overlap with dozens of other common illnesses. Influenza, bacterial meningitis, even a bad summer cold can look similar in the early stages. There’s no rapid at-home test like there is for COVID-19.
When to See a Doctor Immediately
If you develop any of the following after spending time outdoors during mosquito season — especially in an area with known WNV activity — seek medical care urgently:
- Sudden confusion or disorientation
- Stiff neck combined with high fever
- Seizures or uncontrolled muscle tremors
- Muscle weakness or paralysis in one or more limbs
- Loss of vision or extreme sensitivity to light
These are neurological red flags. Don’t wait them out.
Diagnostic Tests Your Doctor May Order
Diagnosis typically involves blood or cerebrospinal fluid (CSF) tests. The standard approach:
- IgM antibody tests (ELISA) — detects antibodies your immune system has made against the virus. Usually detectable 3–8 days after symptom onset.
- Plaque reduction neutralization test (PRNT) — more specific, used to confirm IgM-positive results or distinguish WNV from other flaviviruses.
- PCR testing — detects viral RNA directly, but the window is narrow since the virus clears from blood quickly.
- CSF analysis — if neurological symptoms are present, a lumbar puncture may be performed to examine cerebrospinal fluid.
There’s no antiviral drug that specifically targets West Nile virus. Treatment is supportive — managing fever, maintaining hydration, controlling seizures if they occur, and in serious cases, intensive care. Several antiviral candidates have been studied, but none have yet demonstrated sufficient clinical efficacy to gain approval.
Who Is Most at Risk for Severe West Nile Virus Symptoms?
Not everyone who gets infected faces the same risk profile. Age and immune status are the two dominant factors — and the data here is pretty stark.
| Risk Factor | Why It Increases Risk | Level of Risk |
|---|---|---|
| Age 60+ | Immune system less capable of containing neurotropic viruses | High |
| Organ transplant recipients | Immunosuppressive drugs blunt viral defense | Very High |
| Cancer patients on chemotherapy | Compromised immune surveillance | High |
| HIV/AIDS (advanced) | CD4+ T-cell depletion limits viral clearance | High |
| Diabetes (Type 2) | Associated with chronic inflammation; may impair CNS defense | Moderate-High |
| Hypertension | Emerging research links to poorer outcomes | Moderate |
| Healthy adults under 50 | Robust immune response typically controls infection | Low (but not zero) |
A 2010 study published in Emerging Infectious Diseases found that adults over 70 were 43 times more likely to develop neuroinvasive disease compared to those under 50. That number stuck with me when I first read it. Forty-three times. Prevention for elderly family members isn’t optional — it’s genuinely important.
Neuroinvasive WNV Risk
Rises Sharply with Age
vs. those under 50
Adults 70+ face 43× higher risk of neuroinvasive disease than adults under 50, including encephalitis and acute flaccid paralysis.
Immunocompromised individuals at any age (transplant recipients, chemotherapy patients) have Very High risk regardless of age bracket.
Healthy adults under 50 rarely progress to neuroinvasive disease — but asymptomatic infection still occurs in this group.
10% mortality rate in documented neuroinvasive cases; ~50% of acute flaccid paralysis patients retain persistent weakness years later.
Source: Hayes et al. (2005) Emerging Infectious Diseases; Petersen et al. (2013) JAMA; CDC WNV Surveillance Data 1999–2024
Geographic and Seasonal Risk Factors
West Nile virus peaks in late summer — typically August and September in most of the US — when Culex mosquito populations are at their highest and have had the entire summer to feed on infected birds. The risk doesn’t just depend on geography; local conditions matter enormously.
- States with the highest historical burden: Texas, California, Colorado, South Dakota, Nebraska
- Urban areas with stagnant water (catch basins, poorly maintained storm drains) can sustain large Culex populations even in dry years
- Dead bird sightings — particularly dead crows and jays — are a sentinel indicator of active WNV transmission in your area
- Check your local health department’s WNV surveillance data; many counties publish weekly updates during peak season
How to Avoid West Nile Virus: Evidence-Based Protection Strategies
I’ll be direct: there is no vaccine for humans. One exists for horses — West Nile-Innovator from Zoetis has been available since 2003 — but human vaccine development has stalled despite promising candidates. Until that changes, prevention comes down to mosquito avoidance and environmental management.
1. Personal Protection: What Actually Works
Not all repellents are equal. The EPA registers active ingredients based on efficacy and safety data. Here’s what the science supports:
| Active Ingredient | Efficacy Against Culex | Duration of Protection | Notes |
|---|---|---|---|
| DEET (20–30%) | Excellent | 4–8 hours | Gold standard; safe for adults and children 2 months+ |
| Picaridin (20%) | Excellent | Up to 8 hours | Odorless, less greasy than DEET; growing in popularity |
| IR3535 (20%) | Good | 2–4 hours | Gentle on skin; suitable for sensitive individuals |
| Oil of Lemon Eucalyptus (OLE) | Good | Up to 6 hours | Plant-derived; NOT for children under 3 |
| 2-Undecanone | Moderate | 2–4 hours | Newer, plant-based option; less data available |
| Citronella products | Poor | 30–45 minutes | Not recommended as primary protection |
Apply repellent to all exposed skin. Don’t skip the neck and ankles — Culex mosquitoes often bite low on the body. If you’re using both sunscreen and repellent, apply sunscreen first, let it absorb, then apply repellent on top.
Which Mosquito Repellent Actually Works?
EPA-registered active ingredients ranked by efficacy against Culex mosquitoes (primary WNV vector) — concentration at recommended dosage
Apply repellent after sunscreen. Focus on neck, ankles, and wrists — Culex mosquitoes prefer low-body bites near dusk and dawn.
Source: US EPA Repellent Finder; CDC Vector Control Division; American Mosquito Control Association
2. Protective Clothing and Timing
Since Culex mosquitoes are most active at dusk and dawn, scheduling outdoor activities outside those windows reduces exposure significantly. When you are outside during peak hours:
- Wear long-sleeved shirts and long pants — lightweight, breathable fabrics in hot weather
- Permethrin-treated clothing provides additional protection; it kills mosquitoes on contact and survives multiple washes
- Light-colored clothing makes mosquitoes slightly easier to spot before they bite
- Tuck pants into socks when in heavily vegetated areas
3. Eliminating Standing Water: The Most Underrated Prevention Step
I spent a weekend one summer doing a full sweep of my property, and the amount of standing water I found was genuinely embarrassing. Old flower pot saucers. A tarp folded in the corner of the yard. A clogged rain gutter I hadn’t noticed. These are Culex mosquito nurseries.
Culex pipiens completes its larval development in as little as 7–10 days in warm water. That means standing water after a rainstorm can produce biting mosquitoes within a week and a half. The practical steps:
- Empty and scrub bird baths every 3–4 days — scrubbing removes the eggs, which can be drought-resistant
- Change pet water bowls daily
- Drill drainage holes in the bottom of flower pot saucers — or switch to elevated pot feet
- Keep gutters clean and well-sloped so water doesn’t pool
- Store tarps and equipment so they don’t collect water
- Treat ornamental ponds and rain barrels with Bacillus thuringiensis israelensis (Bti) — a naturally occurring bacterium that kills mosquito larvae without harming birds, fish, or beneficial insects
- Report clogged storm drains to your municipality — these are major Culex breeding sites in urban neighborhoods
4. Home Defense: Screens, Fans, and Environmental Controls
Keep window and door screens in good repair — it sounds obvious but a single torn screen can let in dozens of mosquitoes. If you sleep with windows open, make sure screens fit tightly. Ceiling fans and floor fans create air movement that physically impedes mosquitoes; they’re weak fliers and struggle against even moderate air currents.
Mosquito traps like the Mega-Catch and BG-Sentinel can reduce local populations in yards, though they work best as supplements to elimination measures, not replacements. CO₂-emitting traps are more effective than UV-only models since mosquitoes primarily locate hosts via carbon dioxide and body heat.
5. Community-Level Control: Larviciding and Adulticiding
Individual action matters, but West Nile virus is also a public health issue requiring coordinated response. Most counties in endemic areas operate mosquito control programs that include:
- Larviciding — applying Bti or methoprene (insect growth regulator) to standing water bodies that can’t be eliminated
- Adulticiding — aerial or truck-mounted spraying of pyrethrin or permethrin during outbreak conditions. These operations are carefully timed and targeted; the public health benefit in high-transmission scenarios generally outweighs the limited environmental impact
- Surveillance programs — trap networks and dead bird reporting systems that track viral activity and guide intervention decisions
If your community has a mosquito control district, report standing water issues on public property and sign up for their alerts. These programs genuinely work when they’re funded and properly implemented.
Vulnerable Groups: Protecting Those at Highest Risk
1. For Older Adults
If you’re over 60 — or if you have elderly parents or grandparents — the prevention calculus is different. Repellent use becomes non-negotiable during outdoor activities in peak season. Consider mosquito netting for sleeping if there’s any chance of indoor mosquitoes. Talk to a physician about individual risk, especially if there are underlying immune-compromising conditions.
2. For Immunocompromised Individuals
Organ transplant recipients, people receiving chemotherapy, and anyone on long-term immunosuppressive therapy should be aware that their risk of neuroinvasive disease is substantially elevated. Some transplant centers actively counsel patients on WNV during mosquito season and adjust surveillance accordingly.
3. For Pregnant Women
The evidence for intrauterine transmission is limited but documented. The CDC recommends that pregnant women follow all standard protective measures. If fever and neurological symptoms develop during pregnancy, immediate evaluation is warranted.
West Nile Virus – Seasonal Heatmap
12-month activity heatmap covering mosquito activity, bird amplification, human risk, CDC cases, and prevention priority.
When Is West Nile Virus
Transmission Season?
Source: CDC ArboNET Surveillance; AMCA Seasonal Activity Data; entomological field observation
West Nile Virus in Context: What the Research Actually Shows
A few data points worth having in your head:
- Since 1999, the CDC has recorded over 60,000 reported cases of West Nile virus in the US — but estimates of actual infections (including asymptomatic cases) range into the millions.
- In bad years — 2012 was particularly severe with over 5,000 reported cases — outbreaks can strain local healthcare capacity.
- Climate modeling suggests that warming temperatures and changing precipitation patterns are expanding the range and extending the season for Culex mosquitoes. WNV is not going away.
- The 10-year survival analysis of neuroinvasive WNV cases shows approximately 10% mortality, with many survivors experiencing lasting neurological deficits.
The science is clear: this virus is serious. But it’s also largely preventable through consistent application of the measures described in this guide.
Conclusion: Stay Informed, Stay Protected
West Nile virus isn’t the kind of threat that gets dramatized on the evening news the way Ebola or Zika do. It operates quietly, season after season, mostly invisible. That invisibility is actually part of the problem — it breeds complacency.
Understanding west nile virus symptoms — from the mild fever to the rare but devastating neuroinvasive forms — puts you in a position to act appropriately if you or someone you care about gets sick. Knowing how to recognize early warning signs, how to know if you have west nile virus, and when to seek urgent care can genuinely change outcomes.
The good news is that the protective measures work. Repellent use, eliminating standing water, timing your outdoor activities — these aren’t complicated interventions. They just require consistency. Every mosquito breeding site you eliminate in your yard is a small but real reduction in local transmission risk.
This past summer I found myself back in my yard, doing that same walkthrough I started doing years ago. Checking gutters, emptying saucers, treating the ornamental pond with Bti. It’s become routine — less anxiety, more habit. My neighbor who was hospitalized recovered, by the way. He still jogs. But he wears long sleeves now at dusk, and he never skips the repellent.
Small changes. Real consequences.