Table of Contents
Introduction
You’re getting ready for a camping trip or heading somewhere tropical where mosquitoes are a genuine concern. You apply a DEET-based repellent — the kind that’s been recommended by travel clinics and public health agencies for decades — and within an hour, something feels wrong. The skin where you applied it is red. It itches. Maybe it burns a little. You wash it off and the irritation slowly fades, but the question lingers: was that a reaction to the DEET or specifically a DEET Allergy?
It’s a situation more people encounter than you’d expect. DEET is the most widely used active ingredient in insect repellents worldwide, which means a large number of people are applying it regularly, and a meaningful subset of them experience some form of skin response. The question is what that response actually means — whether it’s a true allergy, a chemical irritation, something in between, or something else entirely.
The distinction matters. Because how you respond to a DEET reaction depends entirely on what kind of reaction it is. This article examines the science, the symptoms, the causes, and how to manage them responsibly.
What Is DEET and Why It Is Used in Insect Repellents

DEET — N,N-Diethyl-meta-toluamide — is a synthetic compound developed by the U.S. Army in the 1940s and registered for public use in 1957, making it one of the most extensively studied repellent compounds available. It works not by killing insects but by jamming the olfactory receptors they use to detect host cues — carbon dioxide, lactic acid, skin volatiles — which is why it’s effective across mosquitoes, ticks, biting flies, and gnats rather than a single species.
Available in concentrations from 5 to 100 percent, higher concentrations extend protection duration rather than increasing potency. The CDC recognizes DEET alongside picaridin, oil of lemon eucalyptus, and IR3535 as effective repellents — and DEET remains the benchmark against which the others are measured.
Can You Be Allergic to DEET?
Yes — though it’s less common than most people assume when they first notice a skin reaction after application.
The more important clarification is that not all DEET skin reactions are allergic reactions. There are two meaningfully different things that can happen, and they have different causes, different implications, and different management approaches.
Table 1 — Irritant vs Allergic Contact Dermatitis: Key Differences
| Feature | Irritant Contact Dermatitis | Allergic Contact Dermatitis |
|---|---|---|
| Mechanism | Direct chemical barrier damage | Immune-mediated (Type IV hypersensitivity) |
| Requires prior exposure | No — can occur on first contact | Yes — sensitization needed first |
| Onset after exposure | Minutes to 1 hour | 12–72 hours (delayed) |
| Spread beyond application area | Rarely | Common in allergic reactions |
| Worsens with re-exposure | Varies by concentration | Yes — often worsens significantly |
| Who is affected | Anyone, especially sensitive skin | Previously sensitized individuals |
| Resolution after washing | Usually quick | Slower — may persist 48–96 hours |
Irritant Contact Dermatitis
This is the more common of the two. DEET is a chemical solvent — it disrupts the skin’s lipid barrier on contact, particularly at higher concentrations and with repeated exposure. The skin responds to this disruption with redness, mild burning, or itching. This is a direct chemical irritation, not an immune response.
It doesn’t require sensitization over time, it can happen on first exposure, and it tends to correlate with concentration — higher DEET products cause more irritation more readily, particularly on sensitive or compromised skin.
This type of reaction is also more likely on mucous membranes, the face, or areas of thinner skin. It fades relatively quickly after washing the product off and doesn’t indicate that your immune system has mounted a response to DEET specifically.
Allergic Contact Dermatitis
True allergic contact dermatitis involves the immune system. In this type of reaction, the immune system has become sensitized to DEET — typically through repeated exposure — and responds to subsequent contact by triggering a delayed hypersensitivity reaction.
The symptoms are similar to irritant reactions in presentation but tend to appear hours after exposure rather than immediately, may spread beyond the application area, and often worsen with re-exposure even at lower concentrations.
This is a Type IV hypersensitivity reaction, mediated by T-lymphocytes rather than IgE antibodies. It’s the same mechanism behind reactions to poison ivy or nickel jewelry. True DEET allergy in this sense is documented in the dermatological literature but is genuinely uncommon given the scale of DEET use globally.
Rare Systemic Reactions
Urticaria — hives — and systemic allergic responses to DEET have been reported in case studies, though these represent a very small fraction of reported reactions. They involve a broader immune response and warrant prompt medical evaluation. If DEET application is followed by widespread hives, facial swelling, difficulty breathing, or dizziness, that is a medical emergency and requires immediate attention regardless of what caused it.
DEET Allergy Symptoms: What to Look For
Symptoms of a DEET skin reaction vary depending on whether the response is irritant or allergic in nature, and where on the body the product was applied. The most commonly reported include:
- Skin redness and flushing at the application site — typically appearing within minutes to an hour for irritant reactions, or several hours later for allergic contact dermatitis
- Itching — ranging from mild to intense, often worsening if the product is left on the skin
- Burning or stinging sensation — more common with higher concentration products and on thinner or more sensitive skin areas
- Rash — a localized rash at the application site is common in both irritant and allergic reactions; in allergic reactions it may spread beyond the direct contact area
- Hives (urticaria) — raised, itchy welts that may appear at the application site or more broadly across the skin; a less common presentation that suggests a more significant immune response
- Swelling — mild localized swelling can accompany contact dermatitis reactions, particularly around the face or eyes if product was applied nearby
- Blistering — in severe cases of allergic contact dermatitis, small blisters may form at the reaction site; this indicates a significant immune response and warrants medical assessment

Image Credit: Illustration by Author
Symptoms of irritant reactions typically resolve within a few hours of washing the product off. Allergic contact dermatitis symptoms often persist longer and may worsen over 24 to 48 hours before improving. This timeline difference is one of the more useful clinical indicators in distinguishing the two types of reaction.
Table 2 — DEET Allergy Symptoms by Severity
| Severity Level | Symptoms | Reaction Type | Action Required |
|---|---|---|---|
| Mild | Redness, mild itching, flushing at application site | Usually irritant | Wash off, cool compress, monitor |
| Moderate | Persistent rash, burning, significant itching, localized swelling | Irritant or allergic | Wash off, hydrocortisone cream, antihistamine |
| Moderate–Severe | Spreading rash beyond application area, blistering, hives | Likely allergic contact dermatitis | Medical evaluation recommended |
| Severe | Widespread hives, facial swelling, throat tightness, dizziness | Systemic allergic reaction | Emergency medical attention immediately |
What Causes a DEET Skin Reaction?
Understanding why reactions occur helps clarify why some people experience them and others don’t after using the same product.
The Chemical Solvent Effect
DEET is a powerful solvent. It dissolves plastics, synthetic fabrics, and paint — which should give some indication of its chemical activity. On skin, this solvent property disrupts the stratum corneum — the outermost layer of the epidermis that functions as the primary barrier between the body and external environment.
Disrupting this barrier causes localized inflammation. The skin doesn’t need to recognize DEET as a foreign threat to react; it’s responding to the barrier damage itself. This is why irritant reactions don’t require prior exposure.
Immune Sensitization
For a true allergic response to develop, the immune system needs to have encountered DEET previously and mounted a sensitization response — essentially learning to recognize DEET molecules as a target for immune activation. On re-exposure, sensitized T-lymphocytes trigger the inflammatory cascade that produces allergic contact dermatitis symptoms.
This process explains why allergic reactions tend to develop after repeated exposures rather than on first contact, and why people who have used DEET for years without issue can occasionally develop sensitivity over time.
Concentration and Application Frequency
Higher DEET concentrations create greater barrier disruption and expose the skin to more of the compound, increasing the likelihood of both irritant reactions and the accumulation of exposure that can lead to sensitization over time.
Applying DEET multiple times daily, every day, over extended periods — the pattern common in travelers or field workers in endemic regions — represents a meaningfully higher exposure profile than occasional recreational use.
Existing Skin Conditions
People with eczema, psoriasis, or other conditions involving compromised skin barrier function are more susceptible to irritant reactions from DEET because their barrier is already impaired. The same amount of product that produces no reaction in intact skin may cause significant irritation on eczematous skin where the barrier protection is reduced.
Table 3 — DEET Concentration Guide and Skin Risk
| DEET Concentration | Protection Duration | Irritation Risk | Recommended For |
|---|---|---|---|
| 5–10% | ~1–2 hours | Low | Children (over 2 months), sensitive skin |
| 15–25% | ~3–5 hours | Low–Moderate | General adult use, short outdoor activities |
| 30–40% | ~6–8 hours | Moderate | Extended outdoor exposure, hiking, travel |
| 50% | ~8–10 hours | Moderate–High | High-risk regions, prolonged field exposure |
| 75–100% | ~10–12 hours | High | Military, field researchers — not for general use |
Who May Be More Sensitive to DEET
Certain groups have a higher likelihood of experiencing DEET skin reactions, though sensitivity can develop in anyone with sufficient exposure.
- People with sensitive skin or a personal history of contact dermatitis — the skin barrier is more easily disrupted and sensitization may occur more readily.
- Individuals with active eczema, rosacea, or psoriasis — compromised barrier function makes irritant reactions more likely even at low concentrations.
- Children — children’s skin is thinner and more permeable than adult skin, and their barrier function is less robust; this is one reason the American Academy of Pediatrics recommends against using DEET on children under two months and suggests lower concentrations (less than 10%) for older children.
- People who apply DEET frequently and at high concentrations — field workers, military personnel, and frequent travelers to endemic regions accumulate higher cumulative exposure.
- People applying DEET to the face or mucous membranes — thinner skin, greater permeability, and proximity to eyes and nose increase the risk of irritant reactions significantly.
It’s worth being clear that sensitivity doesn’t mean a reaction is inevitable. Many people in all of these categories use DEET without incident. Sensitivity means increased risk, not certainty.
Table 4 — Who Is More at Risk: Sensitivity Factors
| Risk Group | Reason for Increased Sensitivity | Recommended Approach |
|---|---|---|
| Children under 2 months | Skin barrier immature, high permeability | Avoid DEET entirely |
| Children 2 months – 3 years | Thinner skin, developing barrier | Max 10% concentration, limit applications |
| Eczema / psoriasis sufferers | Compromised skin barrier | Use picaridin or IR3535 instead |
| Frequent high-concentration users | Cumulative exposure increases sensitization risk | Rotate to lower concentration or alternative |
| People with contact dermatitis history | Pre-existing sensitization tendency | Patch test or use alternative repellent |
| Facial / mucous membrane application | Thinner skin, greater absorption | Avoid direct application — apply to hands first |
How to Manage a DEET Allergy or Skin Reaction
Immediate Steps
If you notice redness, itching, or burning after applying a DEET product, the first and most important step is to wash the affected area thoroughly with soap and water to remove as much of the product as possible. For most irritant reactions, this alone resolves the discomfort within a short period. Don’t wait to see if it gets worse — remove the product promptly.
- Wash with mild soap and cool water immediately — avoid hot water, which increases skin vasodilation and may worsen the reaction.
- Remove any clothing that may have had product applied to it — DEET can remain active on fabric.
- Avoid rubbing the area — patting dry reduces further mechanical irritation to already sensitized skin.
- Apply a cool compress if burning or itching persists after washing — this helps reduce localized inflammation.
- Over-the-counter hydrocortisone cream (1%) can help reduce inflammation in mild contact dermatitis reactions — apply thinly to the affected area.
- Oral antihistamines may help manage itching in both irritant and allergic reactions — cetirizine or loratadine are commonly used options.
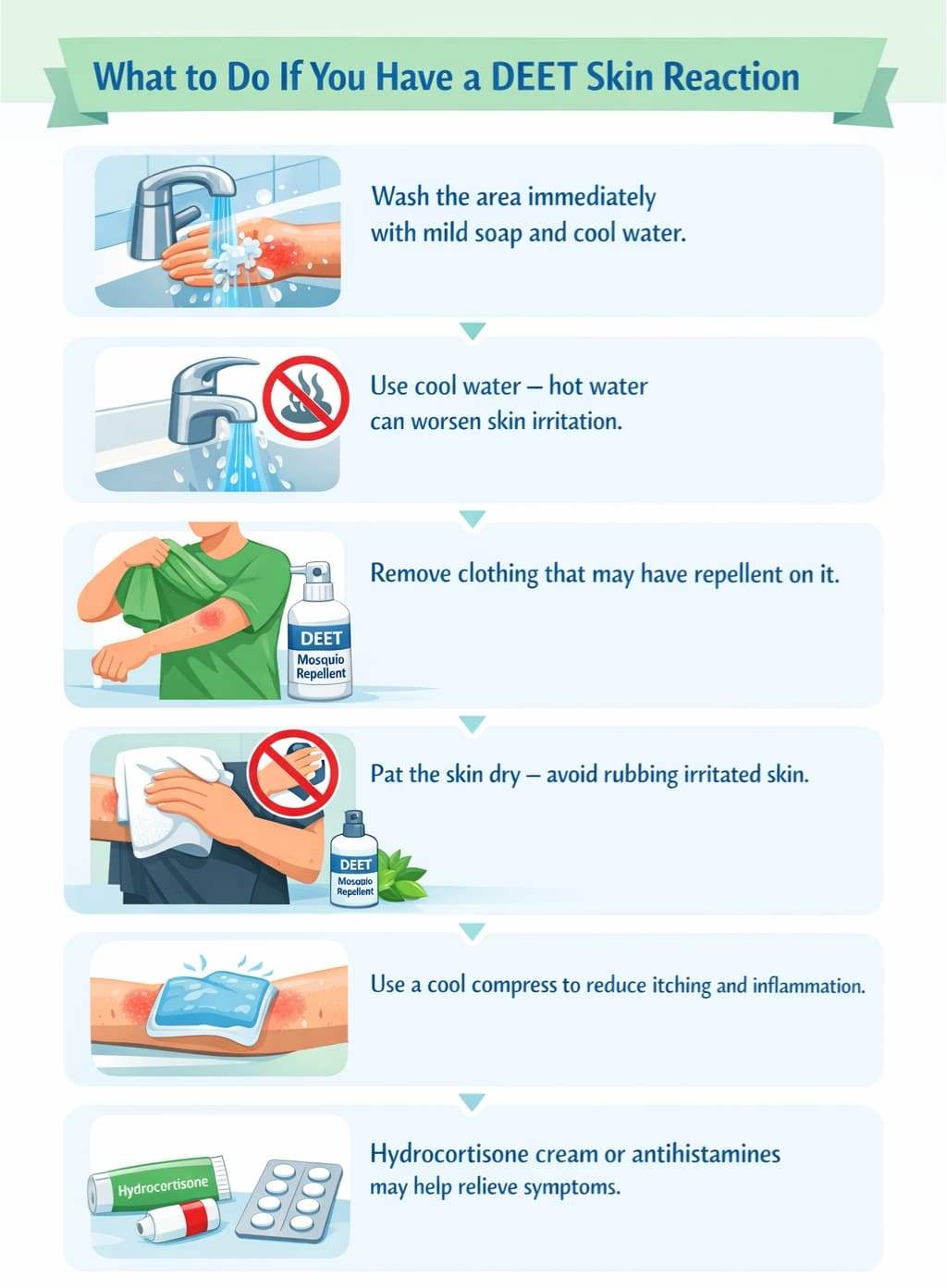
Image Credit: Illustration by Author
When to Seek Medical Attention
Some reactions require professional evaluation rather than home management.
- Symptoms that worsen significantly over 24 to 48 hours despite washing the product off
- Blistering or significant swelling at the reaction site
- Widespread hives or rash spreading beyond the application area
- Any symptoms suggesting a systemic reaction — facial swelling, throat tightness, difficulty breathing, dizziness — which require emergency evaluation immediately
- Reactions in young children that don’t resolve quickly after product removal
A dermatologist can perform patch testing to confirm whether a true contact allergy to DEET exists. This involves applying small amounts of the compound under controlled conditions and observing the skin response over 48 to 96 hours. Confirmation of true DEET allergy has important practical implications for future travel and mosquito protection planning.
Alternative Repellents for Sensitive Individuals
If you’ve had a confirmed or suspected DEET reaction, several effective alternatives exist. Picaridin — also known as icaridin — has a comparable efficacy profile to DEET and a substantially lower rate of skin irritation. It’s odorless, doesn’t dissolve plastics, and is well-tolerated by people who find DEET irritating.
Oil of lemon eucalyptus (OLE) and its synthesized equivalent PMD are plant-derived options with documented repellent activity, though they are not recommended for children under three. IR3535 is another synthetic option with a good skin tolerance profile.
The CDC recognizes all of these as effective alternatives. Switching repellent active ingredient rather than abandoning repellent use entirely is the responsible approach — particularly for travel to regions with meaningful mosquito-borne disease risk.
Table 5 — DEET Alternatives for Sensitive Individuals
| Repellent | Active Ingredient | Skin Tolerance | Protection Duration | CDC Recognized | Notes |
|---|---|---|---|---|---|
| Picaridin | Icaridin | Excellent — low irritation | 8–14 hours | Yes | Closest efficacy match to DEET |
| Oil of Lemon Eucalyptus | PMD (synthesized) | Good | 6–8 hours | Yes | Not for children under 3 |
| IR3535 | Ethyl butylacetylaminopropionate | Very good | 4–8 hours | Yes | Common in European products |
| Permethrin | Permethrin | Good — for clothing only | Weeks (on fabric) | Yes | Not for direct skin application |
| 2-Undecanone | Methyl nonyl ketone | Good | 4–5 hours | Yes | Plant-derived, newer option |
Allergic Reaction to DEET: Symptoms to Recognize
An allergic reaction to DEET presents differently from simple skin irritation, and knowing the difference matters — both for how you respond in the moment and for what you do about future repellent use. The defining feature of a true allergic reaction to DEET is immune system involvement.
The skin doesn’t just react to chemical contact; it mounts a targeted response because it has been sensitized to DEET through prior exposure and now treats it as a foreign threat.
The symptoms of an allergic reaction to DEET typically appear several hours after application rather than immediately — a delayed onset that distinguishes allergic contact dermatitis from the faster irritant response. Common presentations include a red, itchy rash at the application site that may spread beyond the area of direct contact, raised welts or hives, localized swelling, and in some cases blistering.
The rash often feels more intense than irritant reactions and tends to persist longer even after the product has been washed off.
An allergic reaction to DEET bug spray specifically — rather than cream or lotion formulations — can be complicated by the presence of alcohol propellants and fragrance compounds in spray products, either of which may independently trigger or amplify the skin response.
If you react to a DEET bug spray but have previously tolerated other DEET formats without issue, the formulation rather than the active ingredient may be the primary culprit. Switching formulation type is a reasonable first step before concluding a DEET allergy exists.
Symptoms that go beyond localized skin response — widespread hives, swelling of the face or throat, difficulty breathing, dizziness — indicate a systemic allergic reaction rather than contact dermatitis. This level of response requires emergency medical attention immediately, not home management.
Table 6 — Comparison across Irritant, Allergic, and Systemic reactions
| Symptom | Irritant Reaction | Allergic Reaction (DEET) | Systemic Reaction |
| Onset after exposure | Minutes to 1 hour | 6–24 hours (delayed) | Minutes to 2 hours |
| Redness / flushing | Yes — at application site | Yes — may spread beyond site | Widespread |
| Itching | Mild to moderate | Moderate to intense | Intense, widespread |
| Rash / hives | Localized rash | Spreading rash, possible blisters | Hives over large areas |
| Swelling | Mild, localized | Localized to moderate | Face, throat — severe |
| Breathing difficulty | No | No | Yes — emergency |
| Spreads beyond contact area | Rarely | Commonly | Yes |
| Resolves after washing off | Usually within hours | May persist 48–96 hours | Requires emergency care |
| Action required | Wash off, monitor | Wash off, treat, see doctor if worsening | Call emergency services immediately |
How to Treat an Allergic Reaction to DEET
How you treat an allergic reaction to DEET depends on the severity and type of reaction. The steps differ between a localized skin response and a systemic reaction, and conflating the two leads to either under-treatment of something serious or unnecessary alarm over something manageable.
For localized allergic contact dermatitis — rash, itching, swelling confined to the application area — the first step is thorough washing. Remove as much DEET as possible with mild soap and cool water immediately. Don’t use hot water, which increases vasodilation and can worsen the inflammatory response. Remove any clothing the product was applied to or that came into contact with treated skin, as DEET remains active on fabric.
- Wash the affected area with mild soap and cool water as soon as a reaction is noticed — prompt removal reduces the duration and intensity of the response
- Apply a cool compress to the area to reduce localized inflammation and relieve burning or itching
- Over-the-counter 1% hydrocortisone cream applied thinly to the rash helps reduce immune-mediated inflammation — use twice daily for no more than seven days without medical guidance
- Oral antihistamines — cetirizine (Zyrtec) or loratadine (Claritin) — help control itching and mild hive reactions; diphenhydramine (Benadryl) is more sedating but effective for acute reactions
- Avoid scratching — broken skin from scratching increases infection risk and prolongs healing
- Do not reapply DEET or any product containing DEET while the reaction is active
If symptoms worsen significantly over 24 to 48 hours despite these measures, or if blistering develops, a dermatologist visit is appropriate. They may prescribe a short course of topical or oral corticosteroids for more significant allergic contact dermatitis — over-the-counter hydrocortisone is often insufficient for a confirmed immune-mediated reaction.
For any systemic symptoms — throat tightening, difficulty breathing, widespread hives beyond the application area, facial swelling, or dizziness — do not attempt home treatment. Call emergency services immediately. If the person has a known severe allergy and carries an epinephrine auto-injector, use it and still seek emergency care. A systemic allergic reaction to DEET is rare but constitutes a medical emergency when it occurs.
Once the acute reaction resolves, the practical next step is patch testing with a dermatologist to confirm whether the reaction was specifically to DEET or to another ingredient in the formulation. That confirmation determines whether all DEET products should be avoided or whether a different formulation or an alternative active ingredient is sufficient going forward.
Table 7 — 3-Tier Severity Vs Treatment Process
| Severity | Symptoms | Home Treatment | Medical Care Needed? |
| Mild — Irritant | Redness, mild itch, flushing at site | Wash off, cool compress, monitor | No — unless persists beyond 24 hrs |
| Moderate — Allergic | Spreading rash, intense itch, swelling, blistering | Hydrocortisone 1%, antihistamines, no re-exposure | Yes — dermatologist if worsening |
| Severe — Systemic | Hives, facial/throat swelling, breathing difficulty, dizziness | Use epinephrine auto-injector if available | Emergency services immediately |
Wash with mild soap & cool water · Remove treated clothing
throat tightening · facial swelling · breathing difficulty · dizziness · widespread hives
- Use epinephrine auto-injector if available
- Do not drive — wait for emergency services
- Tell medical staff DEET was applied and when
- Cool compress to reduce inflammation
- Hydrocortisone 1% cream — thin layer twice daily
- Antihistamine: cetirizine or loratadine
- Do not scratch — do not reapply DEET
- See doctor if no improvement after 48 hrs
- Take antihistamine immediately
- See dermatologist — likely allergic contact dermatitis
- Prescription corticosteroid may be required
- Request patch testing to confirm DEET allergy
- Switch to picaridin or IR3535 going forward
Identifies whether DEET or an inactive ingredient is responsible — determines your future repellent choice.
DEET Allergy: Understanding the Full Spectrum of Allergic Reactions to DEET
DEET allergy is a term that gets used loosely, and that looseness creates real confusion. In the strictest clinical sense, a DEET allergy refers to an immune-mediated hypersensitivity response — the skin or body recognizing DEET as a threat and mounting a defensive reaction.
But in everyday usage, people describe any unpleasant skin response to DEET-based products as a DEET allergy, which bundles together reactions with very different causes and implications.
True DEET allergy — specifically allergic contact dermatitis — is documented but uncommon relative to the scale of DEET use globally. What is considerably more common is irritant contact dermatitis: a direct chemical reaction to DEET’s solvent properties that doesn’t involve the immune system at all.
Both produce redness, itching, and discomfort. Both are real. But only one is a genuine allergy in the immunological sense.
The reason this distinction matters is practical. If your reaction is irritant-based, switching to a lower DEET concentration or applying it to clothing rather than skin often resolves the problem.
If your reaction is a true DEET allergy, re-exposure at any concentration is likely to trigger the same or worsening response, and switching to an alternative active ingredient is the appropriate path. Getting that diagnosis right — ideally through patch testing with a dermatologist — determines what your next steps should be.
Allergy to Mosquito Repellent: Is It Always the DEET?
When someone develops a reaction after applying mosquito repellent, DEET is the instinctive suspect — but it isn’t always the cause. Most commercial insect repellent formulations contain multiple ingredients beyond the active repellent compound: preservatives, emulsifiers, fragrance compounds, skin conditioning agents, and alcohol carriers.
Any of these can independently trigger a skin reaction in sensitive individuals, and reactions to these inactive ingredients are likely underreported because the product as a whole gets blamed rather than the specific component causing the response.
Fragrances are among the most common contact allergens in personal care products, including repellent sprays and lotions. Preservatives such as parabens and methylisothiazolinone — present in many cosmetic and topical formulations — are well-documented sensitizers.
If you have experienced what seems like an allergy to mosquito repellent but tolerate DEET-containing products in different formulations without issue, an inactive ingredient is a plausible culprit worth investigating.
Patch testing by a dermatologist can identify exactly which component is responsible — testing individual ingredients rather than the product as a whole. An allergy to mosquito repellent as a broad category is far less common than sensitivity to one specific ingredient in one specific formulation. That distinction matters practically: it may mean switching brand rather than abandoning DEET entirely.
DEET Poisoning: When Exposure Goes Beyond a Skin Reaction
DEET poisoning — also called DEET toxicity — is distinct from contact dermatitis and considerably more serious. It refers to systemic toxicity from excessive skin absorption, accidental ingestion, or repeated high-concentration application resulting in neurological effects.
The neurological system is the primary concern: case reports document seizures, encephalopathy, and central nervous system effects, most commonly in young children where skin permeability is higher and body mass relative to dose is lower.
Symptoms that indicate DEET poisoning rather than a skin reaction include:
- Confusion or disorientation
- Slurred speech or tremors
- Seizures or loss of consciousness
- Ingestion of any amount by a child — contact Poison Control immediately at 1-800-222-1222
These require emergency medical attention, not home management. They are categorically different from localized rash or irritation.
Preventing DEET poisoning comes down to correct usage:
- Apply only to exposed skin — not under clothing
- Never apply to children’s hands
- Use age-appropriate concentrations (max 10% for young children)
- Avoid application to broken or irritated skin
- Wash off when returning indoors
DEET used within labeled guidelines carries an extensive safety record. The risk is in misuse — particularly with children — not in the compound itself.
📰 Must Read,
✔️ Essential Oils That Repel Mosquitoes Better Than DEET
✔️ Can Mosquito Repellents Cause Skin Rashes?
Final Takeaway: Balancing Protection and Skin Safety
DEET has an extensive safety record built over six decades of widespread use, and the vast majority of people who apply it correctly experience no significant adverse effects. But reactions do happen — irritant contact dermatitis from DEET’s solvent properties is relatively common at higher concentrations, and true allergic contact dermatitis, while less frequent, is real and tends to develop after repeated exposure rather than first contact.
If you consistently react to DEET products, the practical path is patch testing to identify what you’re actually responding to, then trialing an alternative active ingredient that provides equivalent protection. Effective mosquito control without unnecessary skin compromise is achievable for most people — it may just require a different product than the one you started with.
Frequently Asked Questions (FAQs)
Q. Can you suddenly develop a DEET allergy after years of using it without problems?
Yes — sensitization can develop gradually through repeated exposure, meaning the immune system can learn to recognize DEET as a target at any point. The first reaction often feels surprising precisely because prior tolerance felt like proof of safety. If you’ve used DEET for years without issue and suddenly develop a rash, that timeline is actually consistent with how allergic contact dermatitis works.
Q. Is DEET safe for children or should parents avoid it?
DEET is considered safe for children over two months when used at appropriate concentrations — the American Academy of Pediatrics recommends 10 percent or lower, applied by an adult and washed off when coming indoors. The concern isn’t DEET itself but misuse: over-application or high concentrations in small children where dose-to-body-mass ratio becomes relevant. For infants under two months, avoid DEET entirely.
Q. What’s the difference between a DEET rash and a mosquito bite reaction?
A DEET reaction appears diffusely across the application area as redness or irritation — not at isolated points. Mosquito bite reactions are discrete raised wheals at specific bite sites, often with a visible central puncture. If the rash spreads evenly over where the repellent was applied rather than appearing as individual bumps, DEET is the more likely cause.
Q. Can DEET cause a reaction on the face or around the eyes?
Facial skin is thinner and more vascular, making it more susceptible to DEET irritation than arms or legs. Direct application near eyes or lips frequently causes irritation even in people who tolerate DEET well elsewhere. Standard guidance is to apply to hands first, then carefully pat onto the face — never spray directly. For facial use, low-concentration DEET or picaridin is the safer choice.
Q. How long does a DEET skin reaction take to clear up?
Irritant reactions typically begin resolving within hours of washing the product off and clear within 24 to 48 hours with basic care. Allergic contact dermatitis takes longer — symptoms often peak at 24 to 48 hours and may persist several days even with hydrocortisone and antihistamines. If significant redness or swelling remains after 72 hours despite home treatment, a dermatologist visit is appropriate.